
OK, quick sum-up for those living in a media-free cave: The US has a resurgence of measles related to falling vaccination rates, especially in specific demographic communities. Ominously, 2015 is starting out with a large, multistate outbreak of measles centered on Disneyland theme parks in California – as of this writing at least 65 epidemiologically linked cases have been identified in 7 US states and Mexico. And of local interest (and concern), a University of Minnesota student was diagnosed with measles this week.
Excellent commentary is available on the internet and in other media regarding measles and the need to improve the public’s acceptance of vaccination in general, and the MMR in particular, to prevent an ongoing spiral of worsening outbreaks of vaccine preventable disease. Just to be clear, there is no epidemiological link between MMR and autism. British gastroenterologist Andrew Wakefield published a fraudulent article in the Lancet in 1998 and then essentially pursued a media campaign to suggest a link between MMR and autism. That article has been wholly discredited. The other authors of the paper withdrew their support and it was retracted. In January, 2010, the UK General Medical Council (essentially the United Kingdom’s medical licensing body), struck Wakefield from the medical register, meting out their harshest sanction available. Unfortunately, Wakefield’s influence has continued to discourage some from vaccinating their children against measles. I have little to add on the above sordid tale, though I encourage readers to know this history because of how significant Wakefield’s impact has been on adherence to recommended vaccinations.
For clinicians, I refer you to the CDC Measles page or the MDH Measles page. I encourage providers who (like myself) have never seen a case of measles (yay! let’s hear it for vaccination!), to review the presenting signs and symptoms of measles as well as your clinic or hospital’s isolation procedures in the event you see a case. You don’t want to be the one contacting the family of someone who was inadvertantly exposed to measles in your healthcare setting.
And let’s get the legal boilerplate out of the way: Yes, I am a doc, but I don’t play one on the internet, so none of what I say should be construed as actual medical advice. Whew!
The topic for today, “What can docs learn about measles from veterinarians?” might seem incongruous as measles is a virus that only infects humans, but let’s talk.

Measles virus belongs to the Paramyxoviridae family of viruses. You have to love virology because the name (Para-“beyond” and -myxo- “slime”) equates to the “beyond slime viruses” and conjures up (at least for me) an image of Bart Simpson working with Petri plates. Viruses in this family have a genome composed of a non-segmented strand of RNA. This contrasts with influenza viruses where the genome is made up of 8 segments (or separate strands of RNA). This difference is important because reassortment of RNA segments between different strains of influenza leads to periodic genetic shifts allowing new pandemics of influenza for which people (and animals) have no immunity. This is one reason why your healthcare provider brings up the flu vaccine every fall. So getting back to the Paramyxoviridae, they have one segment, which gives them genetic stability compared to influenza. Which also means vaccination for measles can be more effective.
Below is a family tree of sorts for this family of viruses – think of it as something you’d find on Ancestry.com, but instead of aunts and uncles, you’ve got viruses that are related to differing degree. The figure here is from an article by Marsh, et al, (looking at a virus not actually that closely related to measles virus, but the image works for our discussion). Take a look at the cluster on the left labeled “Morbilivirus” (sic). Here is where we find measles virus. A number of closely related viruses are in this genus. And except for measles, all the other viruses here are animal pathogens. Very interesting.

This figure shows only the most important morbilliviruses (not all of them). In addition to measles, these include canine distemper (CDV, a pathogen primarily of dogs), peste-des-petits-ruminants (PPRV; I don’t speak French, but obviously it is a pathogen of petite ruminants, i.e., goats and sheep), and then there is rinderpest virus (RPV). Rinderpest virus, the one that strikes terror in animals and people alike. Wait, what? You haven’t heard of rinderpest? Astonishingly, if you are like most folks outside the veterinary or wildlife biology world you’ve probably never heard of it. It’s time to correct that oversight.
One reason for the anonymity of the virus (and the disease of the same name) is that it infects animals, specifically cattle and other members of the Artiodactyla. These are mammals that are even-toed ungulates, including antelope, gazelles, sheep, goats, pigs, and giraffes, among others. The disease has an ancient origin, likely in Asia. As with many diseases, it spread with trade (via the Silk Road) and with human conflicts. The Fifth Plague of ancient Egypt (Exodus 9:1-3) was a cattle plague and may have been rinderpest. The virus is thought to have spread into central Europe in the 13th century with the advancing armies of the Mongols. Starting in the 1700s, multiple well-documented epizootics of rinderpest wracked Europe.
If there ever was an infectious disease candidate for the worst in the world, rinderpest would certainly be in the running. The devastation wrought by the virus seems incomprehensible to us today. Up to 95% of cattle were killed. Famines followed quickly after epidemics of rinderpest because cattle were not only an important source of food (for dairy and meat) but also power (as draft animals used to plow fields).

Rinderpest outbreak in 18th Century Netherlands
Source: Wikipedia
Public Domain
Africa was spared from the disease, until the 1800s. Starting in 1887 the most devastating documented outbreak of rinderpest ensued, when the virus arrived on the continent, home to the world’s largest free ranging population of hooved animals. All essentially susceptible to rinderpest. And then enters the virus. When the Italian military was waging a campaign in Eritrea, they imported cattle from India for food and draft power. Some of the livestock were unfortunately infected with the virus (presumably unbeknownst to the Italians.) The subsequent outbreak in Ethiopia was estimated by contemporary sources to have resulted in 90% mortality of the entire country’s cattle herd. Famine resulted in 1888-1892. A third of the nomadic peoples of East Africa, dependent on hooved animals for milk and protein, are estimated to have died in the viral conflagration.
By 1890, rinderpest had reached Tanzania. In a very small illustration, in the region surrounding Unyanyembe the cattle population fell from a herd of ~40,000 to ~100. Cattle deaths due to the ever-advancing rinderpest were reported in Rhodesia (now Zimbabwe) by 1896 and ultimately the scourge reached all the way to the Cape, killing an estimated 2.5 million head of cattle in southern Africa alone.
And an equal devastation was meted out against wild hooved species. The ecological impacts of rinderpest is a topic worthy of a separate post (and by a guest blogger who is an expert in ecology.) It is hard to comprehend the devastation this plague left in its wake.
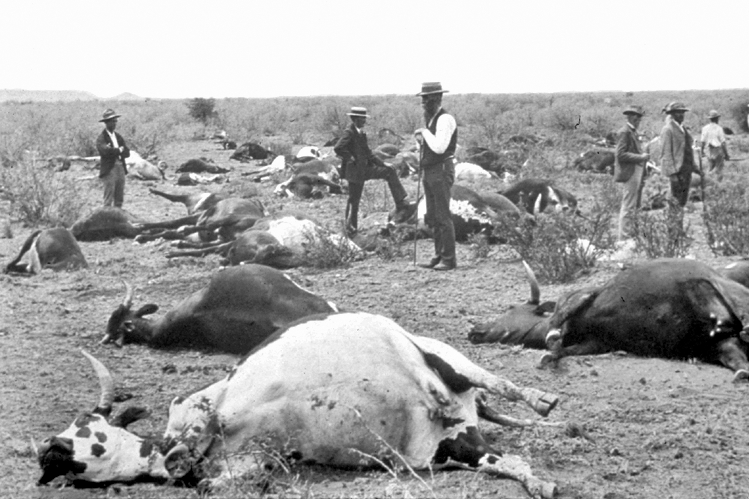
Cows dead from rinderpest in South Africa, 1896. Source: Wikipedia. Public Domain.
Luckily, rinderpest was never imported into North America. And now never will be. A multi-decade effort by wildlife biologists and veterinarians to vaccinate against the plague was ultimately successful. In the case of rinderpest, building herd immunity was both metaphorical and literal. Rinderpest has been eradicated as of May, 2011 – one of only two diseases that can claim the distinction, the other is smallpox.
I want to wrap up this discussion by connecting the rinderpest story back to measles. It turns out measles is not only related to rinderpest – it’s basically it’s offspring. (Imagine the B grade horror flick “Son of Rinderpest.”) Measles appears to have evolved from rinderpest and “jumped” species from cattle to humans around the 11th to 12th centuries. A pandemic ensued that has persisted to this day – most recently impacting Mickey Mouse and his friends.
What can docs learn about measles from veterinarians?
First, this tale is a parable. If rinderpest was eradicated, why not measles? In contrast to measles, rinderpest can infect a variety of host species. Biologists and vets slayed rinderpest in extremely difficult circumstances, working in remote bush across multiple cultural boundaries, during peacetime and war. But the tools used to contain and ultimate eradicate rinderpest were ultimately no different than the public health tools we use against measles.
Second, the story of rinderpest evolving from a virus solely infecting animals to one that infected humans is not unique. In over half of human infectious diseases, the pathogens also infect animals. Of emerging human diseases, the majority ‘jump species’ from an animal host. These include ones that make the headlines: Ebola, SARS, avian and swine influenza… And diseases that don’t: Nipah, Hendra, MERS… Addressing the risks of the next pandemic requires interdisciplinary collaboration between docs and vets as well as ecologists, wildlife biologists, public health sanitarians, and anthropologists. These collaborations have started, but we need to invigorate our approach at transdisciplinary thinking.
#IAMTHEHERD
SUPPLEMENTAL INFORMATION:
For those more interested in the clinical manifestations of rinderpest: A clinical description may be found here.

Rinderpest in cow
Source: CDC PHIL
Public Domain
REFERENCES AND FURTHER READING:
Barrett, T, P Pastoret, & WP Taylor (eds). 2005. Rinderpest and Peste des Petits Ruminants: Virus Plagues of Large and Small Ruminants. Academic Press, Elsevier, London, UK.
Holdo, RM, et al. 2009. A disease-mediated trophic cascade in the Serengeti and its implications for ecosystem C. PLoS Biol 7(9): e1000210. doi: 10.1371/journal.pbio.1000210. (Link)
McNeil, Donald G, Jr. June 28, 2011. Rinderpest, Scourge of Cattle, is Vanquished. New York Times. p D1.
Pankhurst, R. 1966. The great Ethiopian famine of 1888- 1892: A new assessment. J Hist Med 21: 95-124, 271- 293.
Schwabe, Calvin W. 1984. Veterinary Medicine and Human Health. Third Edition. Williams & Wilkins; Baltimore, MD. pp 17- 22.


Pingback: Learning about Measles - Regions Academic Internal Medicine
Nice piece Jonathan– I thought I knew a bit about rinderpest; turns out very little!
LikeLike